







Dyslexia Assessment and Support: What Teachers Need to Know
Learn about dyslexia assessment processes, screening tools (LASS, CTOPP, PhAB, DEST), formal diagnosis pathways, exam access arrangements.


Learn about dyslexia assessment processes, screening tools (LASS, CTOPP, PhAB, DEST), formal diagnosis pathways, exam access arrangements.
Dyslexia affects learners' reading (Shaywitz, 1998). It often appears with ADHD (Barkley, 1990) or visual issues (Stein, 2001). Undiagnosed dyslexia can cause low self-esteem and reading problems (Snowling, 2000). Early identification allows learners to access support at school and work (Elliott & Grigorenko, 2014).

This could help them reframe classroom challenges and provide them with life-long learning strategies. In a Year 4 classroom, a teacher might notice that a learner who gives brilliant verbal answers consistently produces written work full of spelling errors and reversed letters. That pattern, repeated over weeks, is precisely the kind of observation that triggers the assessment pathway described in this guide. We begin by focusing on tests for dyslexia and getting a formal diagnosis. For more on this topic, see Supporting students with dyslexia. Rob Potts then provides practical advice and wisdom accumulated over years of specialist teaching.
Dyslexia assessment falls into two broad categories: screening and diagnostic assessment. These serve different purposes, involve different professionals, and carry different weight in securing support. Understanding which type your learner needs, and when, prevents wasted time and ensures the right intervention begins as early as possible.
Screening is a quick, relatively inexpensive process designed to identify learners at risk of dyslexia. Classroom teachers, SENCOs, or trained teaching assistants can administer most screening tools. A screening result does not constitute a diagnosis, but it provides evidence to support a referral and can trigger targeted classroom interventions immediately. For example, a Year 2 teacher might use the Dyslexia Early Screening Test (DEST-2) during the autumn term to flag learners who need closer monitoring alongside their phonics screening results.
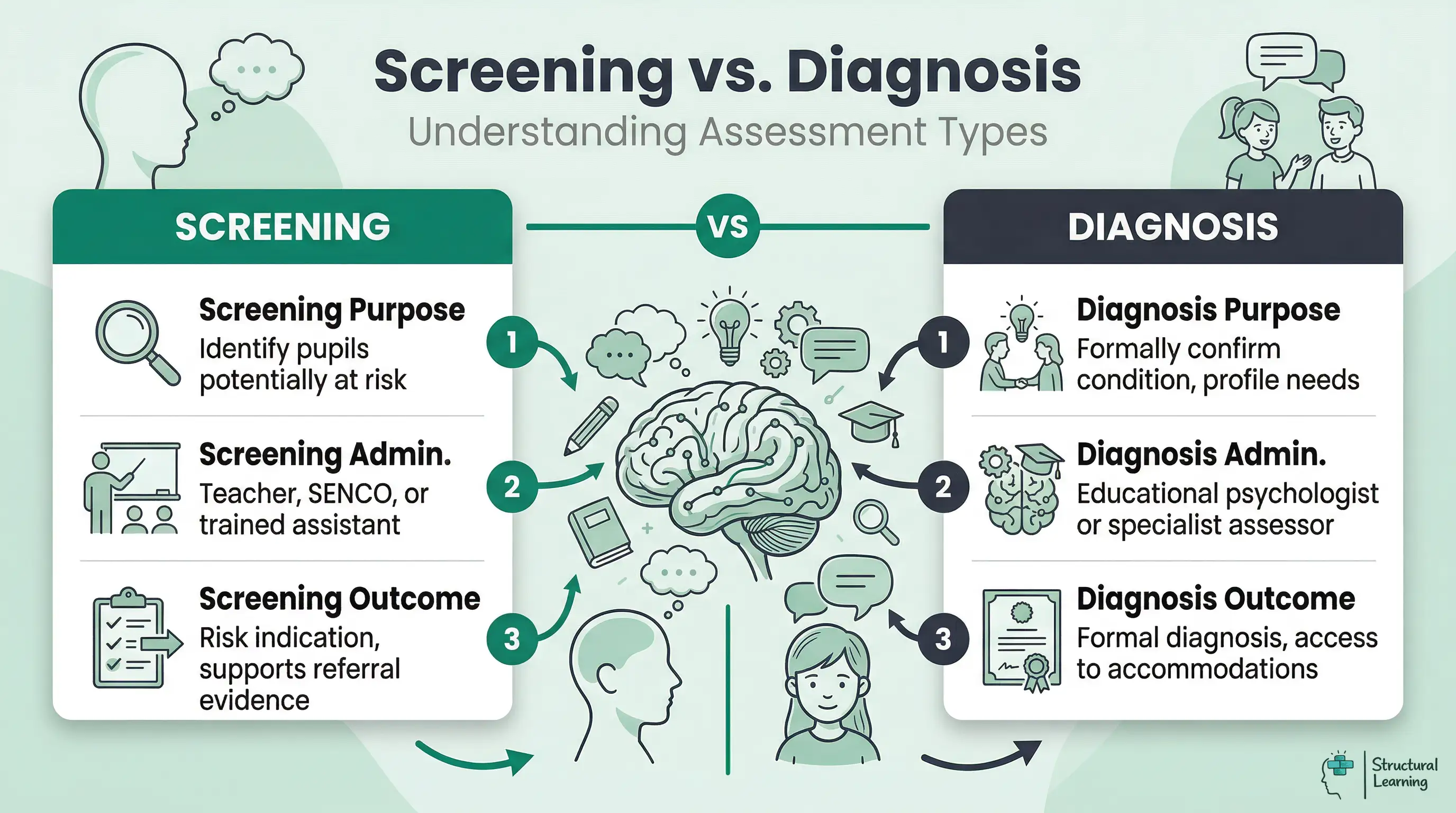
Diagnostic assessment, done by a qualified professional, explores a learner's cognitive skills. It checks phonological awareness, reading fluency, spelling, memory and speed. The detailed profile of strengths and weaknesses helps plan support (e.g. EHCP applications) for the learner (Hulme & Snowling, 2013).
Educational psychologists or specialist assessors (APC) diagnose dyslexia in England and Wales. GPs, teachers, and SENCOs cannot diagnose, but their data informs referrals. Some local authorities offer free assessments; others require schools to pay. Waiting times differ; some areas take weeks, others take over a year.
UK schools draw on a range of standardised screening and assessment tools. Each measures different aspects of reading-related cognition, and the choice depends on the learner's age, the purpose of the assessment, and who will administer it. The table below compares the most widely used instruments.
| Test | Age Range | What It Measures | Who Administers | Approximate Cost |
|---|---|---|---|---|
| LASS (Lucid Assessment System for Schools) | 4 to 15 years | Phonological awareness, memory, phonic decoding, visual-verbal integration | Teacher or SENCO (computer-based) | £400 to £600 for site licence |
| CTOPP-2 (Comprehensive Test of Phonological Processing) | 4 to 24 years | Phonological awareness, phonological memory, rapid naming | Educational psychologist or specialist teacher | £250 to £350 for test kit |
| PhAB-2 (Phonological Assessment Battery) | 5 to 11 years | Alliteration, rhyme, spoonerisms, naming speed, fluency | Teacher, SENCO, or specialist | £200 to £300 for test kit |
| DEST-2 (Dyslexia Early Screening Test) | 4.5 to 6.5 years | Rapid naming, bead threading, postural stability, phonological discrimination, rhyme | Teacher or SENCO | £120 to £180 for test kit |
| WRIT (Wide Range Intelligence Test) | 4 to 85 years | Verbal and visual intelligence, general cognitive ability (used alongside reading tests) | Educational psychologist | £300 to £450 for test kit |
In practice, most schools begin with LASS or DEST as a screening tool, then refer to an educational psychologist who uses CTOPP-2, PhAB-2, or a broader cognitive battery for formal diagnosis. A Year 3 SENCO might run LASS across all learners flagged by classroom teachers, then use those results to build a case for educational psychology referral for the learners showing the strongest indicators.
A formal dyslexia assessment is not a single test but a structured sequence of activities designed to build a complete picture of how a learner processes language. Understanding this process helps teachers prepare learners and gather the right evidence beforehand.
Assessors check records and family history (e.g., teacher notes). Teachers, compile a portfolio. It should include dated spelling patterns and reading records. Note the learner's response to interventions. A Year 5 teacher might show six months of reversal patterns (e.g. phonics logs).
Next, assess cognitive processing. Measure the learner's working memory, processing speed, and verbal reasoning skills. These tests check if reading difficulties occur with typical cognitive abilities (Elliott & Grigorenko, 2014), possibly indicating dyslexia (Snowling, 2020).
Step 3: Phonological processing assessment. This is the core of dyslexia identification. The assessor tests phoneme segmentation, blending, deletion, and substitution. They also measure rapid automatised naming (RAN), which assesses how quickly the learner can name familiar items such as colours, letters, or digits. Slow RAN speed is one of the strongest predictors of dyslexia (Wolf and Bowers, 1999).
Step 4 assesses literacy. We measure a learner's single word reading (Snowling, 2000). This includes nonword decoding, reading fluency, spelling and writing (Fawcett & Nicolson, 2007). Comparing literacy scores to cognitive scores shows dyslexia patterns (Elliott & Grigorenko, 2014).
Assessors write reports. These reports pinpoint a learner's strengths and weaknesses. They confirm or rule out dyslexia. Reports suggest interventions and support. These reports inform IEPs, provision maps, and exam access requests.
The entire assessment typically takes two to three hours, sometimes split across two sessions for younger learners. Results are usually available within two to four weeks.
Adults often wonder "Am I dyslexic?" after years of unexplained reading difficulties. These learners may have struggled in education, work, or personal lives. Many adults remain undiagnosed.
Dyslexia impacts learners of all ages; specialists diagnose it (Lyon et al., 2003). Begin with a screening test. Discuss results with a specialist. They will assess if symptoms match dyslexia (British Dyslexia Association, 2023).
Specialists use tests like the Grey Oral Reading Test (GOT), Woodcock-Johnson (WJ), and Lindamood (Lindamood & Lindamood, 1969). They assess phonetics and sound awareness for comprehensive learner testing. Refer learners for specialist help when needed.
Some tests assess a child's ability to read rapidly and accurately. The same tests are used to detect dyslexia. A test for dyslexia may assess the following skills.
These are the main tests used to determine reading ability. They can also check rapid automatised naming abilities, a key predictor identified by research (Wolf and Bowers, 1999).
Teachers use assessment findings to inform daily practice after a dyslexia diagnosis. They support each learner’s profile with structured literacy (IDA, 2023). Environmental adjustments and tech are further tools.
Orton-Gillingham approaches are key for dyslexia (British Dyslexia Association). These programmes use explicit, systematic, multisensory teaching. A Year 3 learner might see, hear, trace, and write letter patterns. Programmes should build skills, go step by step, and provide practice.
Coloured overlays and visual stress. Some dyslexic learners experience visual stress where printed text appears to move, blur, or shimmer. Coloured overlays placed over reading material can reduce this effect for some learners. While the evidence base is mixed (Ritchie, Sala, and McIntosh, 2011), overlays are inexpensive and non-invasive, making them worth trialling. A teacher might offer a selection of overlay colours and let the learner choose whichever feels most comfortable for sustained reading.
Assistive technology, like text-to-speech, helps learners with reading and writing. Software and iPad features let dyslexic learners access content. They can work at their level, not just decoding speed. A Year 6 learner can use text-to-speech for science revision. (Read&Write and ClaroRead are helpful tools.)
Adjust the environment. Position the learner away from visual distractions. Give learners handouts instead of board copying. Use dyslexia-friendly fonts (Arial, Comic Sans, or OpenDyslexic). Provide extra time for reading tasks. Scaffolding with graphic organisers, writing frames, and word banks helps learners plan writing.
For learners with dyslexia, examination access arrangements greatly improve results. The Joint Council for Qualifications (JCQ) sets the rules for GCSE and A Level access arrangements in England.
Dyslexic learners often get 25% extra time. Readers, scribes, word processors, and modified papers also help. SENCOs must prove diagnosis and normal classroom use. They also need documented need history (Elliott and Gibbs, 2008).
JCQ needs two evidence sources: formal assessment reports and teacher observations. These observations show learner needs using intervention records and internal data. Schools must apply early, ideally by autumn term. SENCOs should gather evidence at least 18 months beforehand. (JCQ, n.d.)
For younger learners, schools can apply for high needs funding through the local authority to support specialist intervention programmes, one-to-one teaching assistant time, or specialist teacher sessions. An EHCP may be appropriate for learners with severe dyslexia whose needs cannot be met from the school's own SEN budget. Teachers play a critical role in this process by providing detailed evidence of the learner's response to previous interventions and their current level of need.
Identifying dyslexia early is crucial, as it allows for timely intervention and support. Here are strategies teachers can employ.
Dyslexia affects each learner differently. Teachers can support learners with dyslexia. This helps them achieve their potential (Snowling, 2000; Hulme & Snowling, 2013). Appropriate support is key (Reid, 2016; Rose, 2009).
Spotting dyslexia early means seeing persistent issues beyond normal learning. Learners struggle with sounds despite good teaching (Snowling et al.). They might read slowly, spell oddly, or write worse than they speak. These problems often continue even with extra help.
Observe literacy behaviours across contexts. Learners may avoid reading aloud or take longer writing. Good oral skills but poor writing may also appear. Note slow word recognition and letter reversals past age seven. Recall of sight words may be challenging. Bradley and Bryant (1983) showed rapid naming difficulties can signal dyslexia.
Document observations regularly instead of single events. Keep short, dated records with context and support given. This helps discuss learners with SENCOs and supports referrals (Ainscow et al, 2006). Act quickly with differentiated teaching approaches (Florian & Black-Hawkins, 2011).
Researchers Orton and Gillingham found multisensory methods help dyslexic learners. These approaches build literacy by reducing cognitive load. Teachers should present new information in small steps. Learners master each part before moving on.
Dyslexic learners need targeted classroom accommodations for processing differences. Give them more time for reading and writing. They benefit from showing knowledge in other ways (oral presentations, mind maps). Cognitive load theory (Sweller, 1988) suggests simplified worksheets. Use clear fonts (Arial, Comic Sans) and keep formatting consistent.
Explicit phonics is vital daily. Regularly reinforce key ideas and give learners instant feedback. Provide advance organisers and colour-code information. Use both verbal and visual instructions. Encourage literacy risks; see mistakes as chances to learn (Stanovich, 1986; Shaywitz & Shaywitz, 2003).
Refer learners after 6-12 weeks of support if literacy problems continue. Differing oral language skills may suggest dyslexia. Ongoing phonological difficulties are also key. Rose (2009) stresses early identification to improve learner outcomes.
For further reading on this topic, explore our guide to Read Write Inc.
Teachers record learner struggles and what they tried. Collect evidence, like reading and writing samples, plus assessments. Observe learning behaviours in various situations. This helps specialist teachers assess learners. Schools should show classroom support given. Local authorities often ask for this.
Work closely with parents and the SENCO. Keep records of interventions and progress for assessments. This data helps plan support (Vaughn & Fuchs, 2003). Early talks with families and good records speed things up (Sailor, 2009; Turnbull et al., 2011).
Research on collaborative practice consistently shows it supports learners with dyslexia. They showed matching home and school approaches improves reading. Sharing effective plans builds understanding of dyslexia's barriers. Open talks about learner needs remain key.
Communicate assessment results clearly with families. Explain classroom methods, like multisensory phonics (Ehri et al., 2001). Gather family insights on successful strategies at home (Epstein, 2011; Henderson et al., 2007). Note learner preferences and emotional responses too.
Review meetings celebrate progress and tackle challenges together. Teachers help families with homework tips and reading programmes. They also advise on managing frustration during learning at home. When families understand classroom support, learners with dyslexia gain consistent aid (Snowling, 2000; Hulme & Snowling, 2009).
Early identification of dyslexia helps learners. Teachers need to know about assessment and support. Using proper screening tools lets educators provide targeted help. This boosts academic growth and personal skills.
Dyslexia need not hinder success. Learners with dyslexia can thrive if teachers provide effective support. Use multisensory teaching and assistive tech. Give learners extra processing time. Break tasks into steps (Gillingham & Stillman, 1960). Monitor and adjust support for each learner.
Teachers benefit from professional development and teamwork. Dyslexia awareness training and working with psychologists support learners. Sharing good practice helps colleagues. Strong parent partnerships and clear communication builds learner support.
Rose (2006) showed structured literacy supports all learners. Elliott & Grigorenko (2014) found teachers can build thriving classrooms by helping dyslexic learners. Humphrey & Mullins (2002) discovered this approach encourages positive attitudes to learning.
Screening helps find learners who may need extra support, providing early evidence for interventions. An educational psychologist or specialist teacher with an APC does a full diagnostic assessment. This assessment confirms dyslexia (Elliott & Grigorenko, 2014) and aids applications for an Education, Health and Care Plan (Snowling & Hulme, 2011).
Multisensory learning and coloured overlays help learners access the curriculum. Assistive technology and extra time in assessments support learning (Rose, 2009). Staff should practise these methods regularly to meet individual learner needs (Hattie, 2008; Marzano, 2003).
Teachers can target support early if they identify learning needs (Shaywitz & Shaywitz, 2005). This prevents learner frustration and difficult behaviour. Schools can use early literacy help to tackle phonological problems (Torgesen et al., 1994). This shortens waits for assessments and specialist help (Snowling et al., 2000).
Researchers say structured phonics programmes help learners with dyslexia (Ehri et al., 2001). Addressing working memory aids learners too (Swanson & Alloway, 2008). Small group teaching boosts reading accuracy, studies suggest (Torgesen, 2002).
One common mistake is relying solely on reading tests while ignoring phonological awareness and rapid naming assessments. Teachers may also wait too long to involve the SENCO, which delays the identification process. It is also a mistake to assume that a screening result is a formal diagnosis, as these tools only indicate a level of risk.
Many UK schools use computer-based systems like the Lucid Assessment System for Schools to identify phonological memory and phonic decoding issues. The Dyslexia Early Screening Test is frequently used for younger learners between the ages of four and six. These tools help staff gather data to support a referral to an educational psychologist for a full evaluation.
Free for teachers. Visual schedules, sensory adaptations, low-demand routines, built into the plan.
These studies provide the evidence base for the screening tools and intervention approaches described in this guide.
Identifying Dyslexia: A Review of the Evidence View resource ↗
British Dyslexia Association
British Dyslexia Association (2024)
BDA guidance helps UK schools with screening, diagnosis, and interventions. (BDA, ongoing) It covers learners' literacy. The BDA quality mark accredits programmes meeting strict standards. (BDA, ongoing) These programmes focus on structured literacy teaching.
The Rose Review (2009) highlights identifying learners with dyslexia. It also covers teaching learners who struggle with literacy. The review provides guidance for educators in the UK.
Rose, J. (2009)
The Rose Review (2009) defined dyslexia for the UK government. The review suggested phonics should be the main intervention. It still shapes how schools help learners with dyslexia now.
Improving Literacy in Key Stage 1 View report ↗
EEF Guidance Report
Education Endowment Foundation (2020)
The EEF guidance offers literacy teaching tips. It helps learners who find reading hard. The report (EEF, n.d.) judges methods by research strength and cost.
. Written by leading experts, this book offers a comprehensive, cutting-edge exploration into the multifaceted nature of dyslexia. It meticulously examines the cognitive and neurological underpinnings of reading difficulties, providing invaluable insights into diagnosis and intervention. The text covers phonological processing, orthographic mapping, and reading fluency. It synthesizes research from various perspectives, including cognitive psychology, neuroscience, and education (e.g., Ramus & Szenkovits, 2008; Shaywitz & Shaywitz, 2005; Wolf, Miller, & Donnelly, 2000), offering a truly holistic view of the condition. Furthermore, the book explores effective strategies and interventions that educators can implement to elevate learner outcomes and foster a more inclusive learning environment. It is an indispensable resource for teachers seeking to deepen their understanding of dyslexia and support struggling readers in their classrooms. Rewritten paragraph: "Dyslexia, Reading and the Brain" explores reading difficulties. Leading experts examine cognition and neurology. It aids diagnosis and intervention for learners. Phonological skills and fluency are covered. Research from Ramus & Szenkovits (2008) and others is included. Teachers can use strategies to help learners. Shaywitz & Shaywitz (2005) and Wolf, Miller, & Donnelly (2000) provide extra insight.
Snowling, M. J. (2000, updated 2019)
Snowling (2000) helped shape how we view dyslexia and phonological skills. Her research informs the assessments and interventions teachers use daily. This impacts learner development in UK schools now.
Visual schedules, sensory adaptations, low-demand routines. Built in.



